

Look what they did to our antibodies
Our immune systems are supposed to fight viruses. Now they invite them round for tea. It's all down to IgG4...


Have you heard about the IgG4 antibody switch? It’s been glossed over in official discussions about Covid-19 ‘vaccines’, but it’s the elephant in the room. Let’s break it down and explore why this may matter more than we’re being told.
The antibody switch: what’s the big deal?
Our immune system is like a well-trained army, with different types of antibodies serving as its soldiers. Among them, IgG antibodies are the frontline warriors, designed to neutralize viruses and protect us from infections. But here’s the catch: not all IgG antibodies are created equal. Think of IgG4 antibodies as the peacekeepers of the immune system. They’re not fighters like the other IgG subclasses—they’re more about tolerance, calming things down. They’re certainly not about launching an attack.
Now, here’s where it gets interesting (and worrying).
Studies have shown that repeated Covid-19 mRNA injections—especially after the second dose or booster—cause the body to switch from producing the more effective IgG3 antibodies to producing IgG4. Essentially, the immune system is shifting toward tolerance rather than attack.
Sounds harmless, right? Well, not so fast. Here’s a look at what this shift might mean:
1. More Covid-19 infections
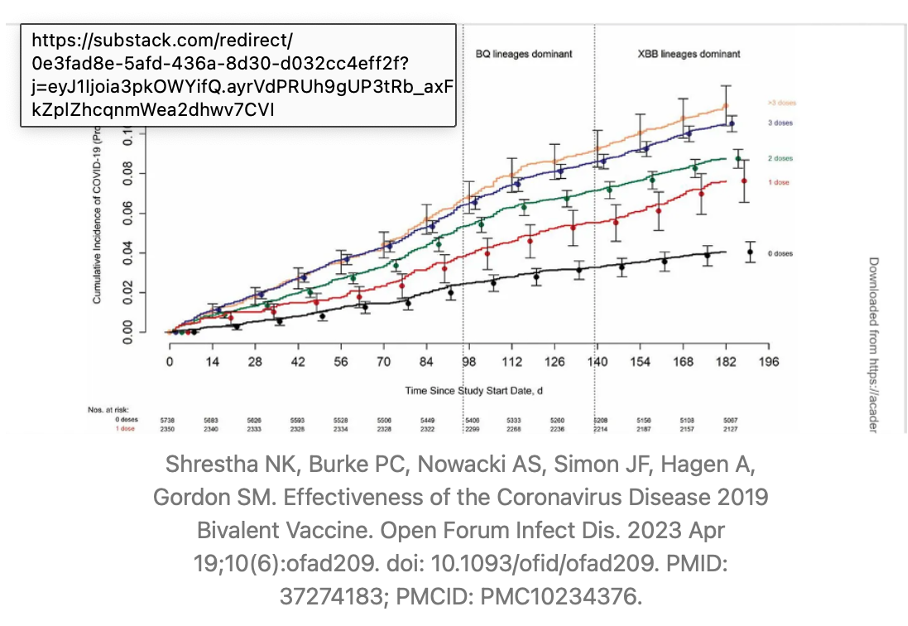
Imagine your immune system being rewired to tolerate the virus instead of fighting it. That’s essentially what the IgG4 switch could entail. A study from the Cleveland Clinic found a troubling trend: the more Covid-19 vaccine doses a person received, the higher their risk of getting infected. This isn’t what we were promised with "safe and effective," is it? The IgG4 antibodies might be making the body less effective at dealing with the virus, leaving vaccinated individuals more susceptible to reinfections.
2. The potential for worse outcomes
IgG4 antibodies are great if you’re dealing with allergies, as they help the body tolerate allergens. But when it comes to fighting a virus like SARS-CoV-2, this tolerance could backfire. Instead of neutralizing the virus, the immune system might let it hang around longer, potentially leading to more severe disease outcomes. It’s like inviting a burglar into your house and offering them tea instead of calling the police.
3. The risk of other conditions
This shift to IgG4 isn’t just about Covid-19. It could open the door to other IgG4-related diseases (known as IgG4-RD). These are a group of conditions where the immune system starts attacking various organs, causing inflammation and fibrosis (thickening or scarring of tissues). Examples include autoimmune pancreatitis, kidney disease, and even conditions affecting the lungs or brain. There have been reports of individuals developing these conditions after receiving the mRNA vaccines. Coincidence? Maybe. But it’s enough to warrant serious investigation.

Pathologies associated with elevated IgG4 levels and IgG4-related diseases
Below is a list of IgG4-related diseases (IgG4-RD) and other pathologies associated with elevated IgG4 levels that could also be related to IgG4 rising after mRNA injections:
Type 1 Autoimmune Pancreatitis (AIP): Chronic inflammation of the pancreas, often presenting with abdominal pain, jaundice, or weight loss. It is one of the most common manifestations of IgG4-RD.
Sialadenitis (Mikulicz’s Disease): Enlargement of the salivary and lacrimal glands, leading to dry mouth and eyes. This is a classic presentation of IgG4-RD in the head and neck region (Stone et al., 2012).
Retroperitoneal Fibrosis: Thickening and fibrosis of the tissue behind the peritoneum, which can lead to ureteral obstruction and kidney damage (Stone et al., 2012).
Riedel’s Thyroiditis: A rare form of thyroiditis involving fibrosis of the thyroid gland. It can present as a hard, fixed thyroid mass that mimics malignancy (Stone et al., 2012).
Küttner’s Tumor (Chronic Sclerosing Sialadenitis): Affects the submandibular glands, causing enlargement and fibrosis, often mistaken for a tumor (Stone et al., 2012).
IgG4-Related Sclerosing Cholangitis: Involves the bile ducts, often associated with autoimmune pancreatitis. Can lead to jaundice and bile duct obstruction (Stone et al., 2012).
IgG4-Related Ophthalmic Disease: Involves orbital inflammation and can cause proptosis (bulging eyes), double vision, or orbital masses (Stone et al., 2012; Uchida et al., 2022).
IgG4-Related Aortitis and Periaortitis: Inflammation of the aorta and surrounding tissues, which may lead to aneurysms or vascular complications (Stone et al., 2012).
IgG4-Related Kidney Disease: Includes tubulointerstitial nephritis and other renal manifestations, leading to kidney dysfunction or masses (Stone et al., 2012; Uchida et al., 2022).
IgG4-Related Lung Disease: Pulmonary involvement, presenting with inflammatory pseudotumors, interstitial pneumonia, or pleural thickening (Stone et al., 2012).
IgG4-Related Lymphadenopathy: Enlargement of lymph nodes that may mimic lymphoma (Stone et al., 2012).
IgG4-Related Skin Disease: While less common, presents as various cutaneous lesions, including plaques or nodules (Stone et al., 2012).
IgG4-Related Prostatitis: Enlargement of the prostate, causing lower urinary tract symptoms (Stone et al., 2012).
IgG4-Related Hypophysitis: Involves inflammation of the pituitary gland, leading to hormonal imbalances such as adrenal insufficiency or diabetes insipidus (Stone et al., 2012).
IgG4-Related Pachymeningitis: Inflammation of the dura mater (the outer membrane covering the brain and spinal cord), leading to headaches, cranial nerve palsies, or other neurological symptoms (Stone et al., 2012).
That’s not all. There are potentially broader implications of elevated IgG4 levels that we must consider:
Repeated infections. Elevated IgG4 levels may impair the immune system’s ability to clear infections, as IgG4 is less effective at neutralizing pathogens (Aalberse, 2009; Irrgang, 2021).
Autoimmune diseases. Elevated IgG4 levels may contribute to autoimmune processes, where the immune system attacks its own tissues (Watad, 2021).
Cancer risks. Chronic inflammation caused by IgG4-related conditions may increase the risk of certain malignancies. While not directly caused by IgG4, this link warrants further research (Uchida, 2022).
Idiopathic Interstitial Lung Disease. Chronic inflammation and fibrosis in the lungs may lead to respiratory symptoms, further complicating the clinical picture (Stone, 2012).
Systemic Vasculitis. Inflammation of blood vessels associated with IgG4-RD can cause systemic complications and end-organ damage (Stone, 2012).
Why isn’t this being talked about?
Good question. The IgG4 switch is a complex phenomenon, and scientists are still trying to figure out its full implications. However, one thing is clear: this isn’t a simple black-and-white issue as the long-term effects of repeated mRNA shots are only now coming into focus.
Health agencies like the CDC and WHO argue that the benefits of vaccination outweigh the risks. But should we ignore potential red flags, especially when they involve changes to our immune system long term? Especially in populations that had virtually no risk from Covid-19 (i.e. children)? Absolutely not.
The science isn’t settled - but nor is this speculation
Elevated IgG4 levels are documented. Multiple studies confirm that repeated mRNA injections lead to a significant increase in IgG4 antibodies (Irrgang et al., 2021). This isn’t speculation—it’s a fact.
Case reports suggest a link. Individuals have developed IgG4-related diseases shortly after getting injected (Uchida et al., 2022). While these cases are rare, as not many practitioners have linked the Covid 19 gene therapy to a certain pathology, they highlight a potential connection that needs further investigation.
The immune response Is complex. The IgG4 switch might be the immune system’s way of adapting to repeated exposure to the spike protein in the vaccines. But this adaptation could come with unintended consequences, including reduced vaccine efficacy and heightened risk of certain diseases. And the most important question is the duration of this fact which we will only know in a decade.
More studies are needed. The science is evolving, and more research is needed to fully understand the implications of this antibody switch. For now, it’s clear that this isn’t a one-size-fits-all situation.
What can we do?
As individuals, the best thing we can do is stay informed. Ask questions if asked to be vaccinated: demand transparency, and weigh the risks and benefits of any medical intervention.
If you yourself have been affected by any of the pathologies above, even months or years after the Covid injections, ask your healthcare providers to assess a potential association. You can test for Covid antibodies (when over 1000 BAU, it is reasonable to assume that you are still producing spike proteins after the injections). You can also get tested for IgG4s (for Covid and generally), for spike proteins (in serum, immune cells, exosomes, body fluids) or for mRNA (in serum, exosomes or any body fluid).
For policymakers and health agencies, it’s crucial to continue monitoring these injections' long-term effects and be honest about potential risks. Ignoring the elephant in the room won’t make it go away.
Final thoughts
The IgG4 switch is an alarming consequence of repeated Covid-19 mRNA vaccinations. The evidence so far suggests that this phenomenon could have significant implications for immunity, vaccine efficacy, and long-term health. It’s time to have an open, honest conversation about those ‘trade-offs’—and to keep the spotlight on the elephant in the room. This is certainly another red flag for the continuation of the Covid 19 gene therapy and adds to the calls for a moratorium of this technology. Especially considering further promotion of mRNA technologies in the US, Europe, and Russia, we urgently need independent scientists to gather at a roundtable with those pushing for even more use. The World Council for Health has repeatedly called for a moratorium on the technology. This is just the latest, essential piece we’re adding to the puzzle.
References
Aalberse, R. C., Stapel, S. O., Schuurman, J., & Rispens, T. (2009). Immunoglobulin G4: an odd antibody. Clinical & Experimental Allergy, 39(4), 469-477. https://doi.org/10.1111/j.1365-2222.2009.03207.x
Bergamaschi, C., Terpos, E., Rosati, M., Angel, M., Bear, J., Stellas, D., ... & Felber, B. K. (2021). Systemic IL-15, IFN-γ, and IP-10/CXCL10 signature associated with effective immune response to SARS-CoV-2 in BNT162b2 mRNA vaccine recipients. Cell Reports, 36(6), 109504. https://doi.org/10.1016/j.celrep.2021.109504
Uchida, K., Ito, S., Nakamura, Y., Hoshino, Y., Abe, Y., Ito, T., ... & Okazaki, K. (2022). IgG4-related disease after BNT162b2 COVID-19 mRNA vaccination: A case report. Vaccine, 40(22), 3079-3082. https://doi.org/10.1016/j.vaccine.2022.04.073
Irrgang, P., Gerling, J., Kocher, K., Lapuente, D., Steininger, P., Habenicht, K., ... & Überla, K. (2021). Class switch towards non-inflammatory, spike-specific IgG4 antibodies after repeated SARS-CoV-2 mRNA vaccination. medRxiv. https://doi.org/10.1101/2022.12.22.22283726
Kang, C. K., Kim, M., Lee, S., Kim, G., Choe, P. G., Park, W. B., ... & Oh, M. D. (2022). Longitudinal analysis of SARS-CoV-2 specific antibody responses after COVID-19 vaccination. Journal of Korean Medical Science, 37(4), e35. https://doi.org/10.3346/jkms.2022.37.e35
Lozano-Ojalvo, D., Camara, C., Lopez-Granados, E., Nozal, P., Del Pino-Molina, L., Bravo-Gallego, L. Y., ... & Paz-Artal, E. (2021). Differential effects of the second SARS-CoV-2 mRNA vaccine dose on T cell immunity in naive and COVID-19 recovered individuals. Cell Reports, 36(8), 109570. https://doi.org/10.1016/j.celrep.2021.109570
Perugino, C. A., AlSalem, S. B., Mattoo, H., Della-Torre, E., Mahajan, V., Ganesh, G., ... & Stone, J. H. (2021). Identification of galectin-3 as an autoantigen in patients with IgG4-related disease. Journal of Allergy and Clinical Immunology, 147(2), 736-745. https://doi.org/10.1016/j.jaci.2020.09.037
Stone, J. H., Zen, Y., & Deshpande, V. (2012). IgG4-related disease. New England Journal of Medicine, 366(6), 539-551. https://doi.org/10.1056/NEJMra1104650
World Health Organization (WHO). (2023). COVID-19 vaccines: safety surveillance manual.
Astonishing how an experimental gene therapy that hadn't been adequately tested was rolled out and treated as a vaccine, and saviour of us all, by the media. I remember how the BBC 6pm news stage-managed the arrival of the mRNA jab as if it was a miracle, with Pharma's rep at the bbc Fergus Walsh "overjoyed" at this great news. As time has gone on one damn bad thing after another about tbe gene therapy has been discovered by independent and public-minded scientists - which the people promoted by the likes of the BBC certainly are not, shame on them. It's depressing that there are such people in the world, and with power, money and influence. The real miracle is the WCH and other independent medics and scientists who have done all they can to point us in the right direction in the face of all those terrible bad actors could throw at them.