
Exposing the WHO Collaborating Centres: new reports reveal institutional encroachment — on an international scale
Two groundbreaking new reports by World Council for Health reveal how the WHO’s presence, policies and systems expand by stealth and become globally entrenched... via a shady system of 'partnerships.'


In December 2025, World Council for Health published an introduction to the WHO Collaborating Centres (CCs): what they are, where they are, what they do — and why their proliferation gives tremendous cause for concern.
Since then, World Council for Health has produced two detailed country-specific reports: USA and UK. These unique reports provide vital insights into the issues surrounding WHO Collaborating Centres: issues which are of grave significance yet up until now have been largely ignored. Both documents can be downloaded here.
Various kinds of organisation can be designated as WHO Collaborating Centres. This includes governmental and public health agencies (such as the CDC and UKHSA), research institutes, hospitals and universities. Notable examples include —among many others— the UK’s Francis Crick Institute, and the US’s Harvard Medical School and Stanford University.
The two reports document which US and UK bodies have WHO Collaborating Centre status (at the time of writing), as well as their terms of reference and scope of activities. CC subject areas span a mind-bogglingly broad spectrum: from cancer to climate change, malaria to mental health.
WHO’s where? Current state of play
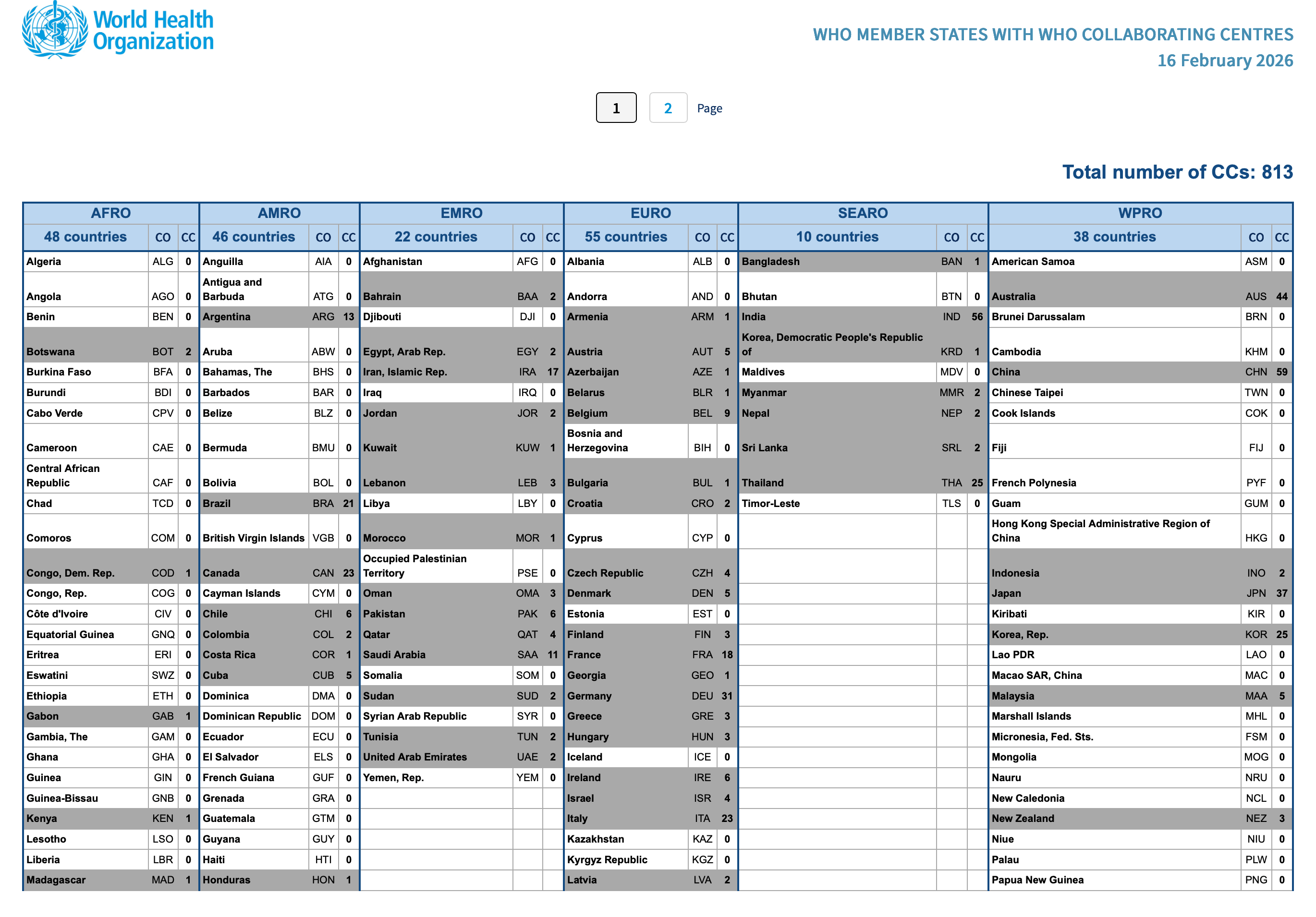
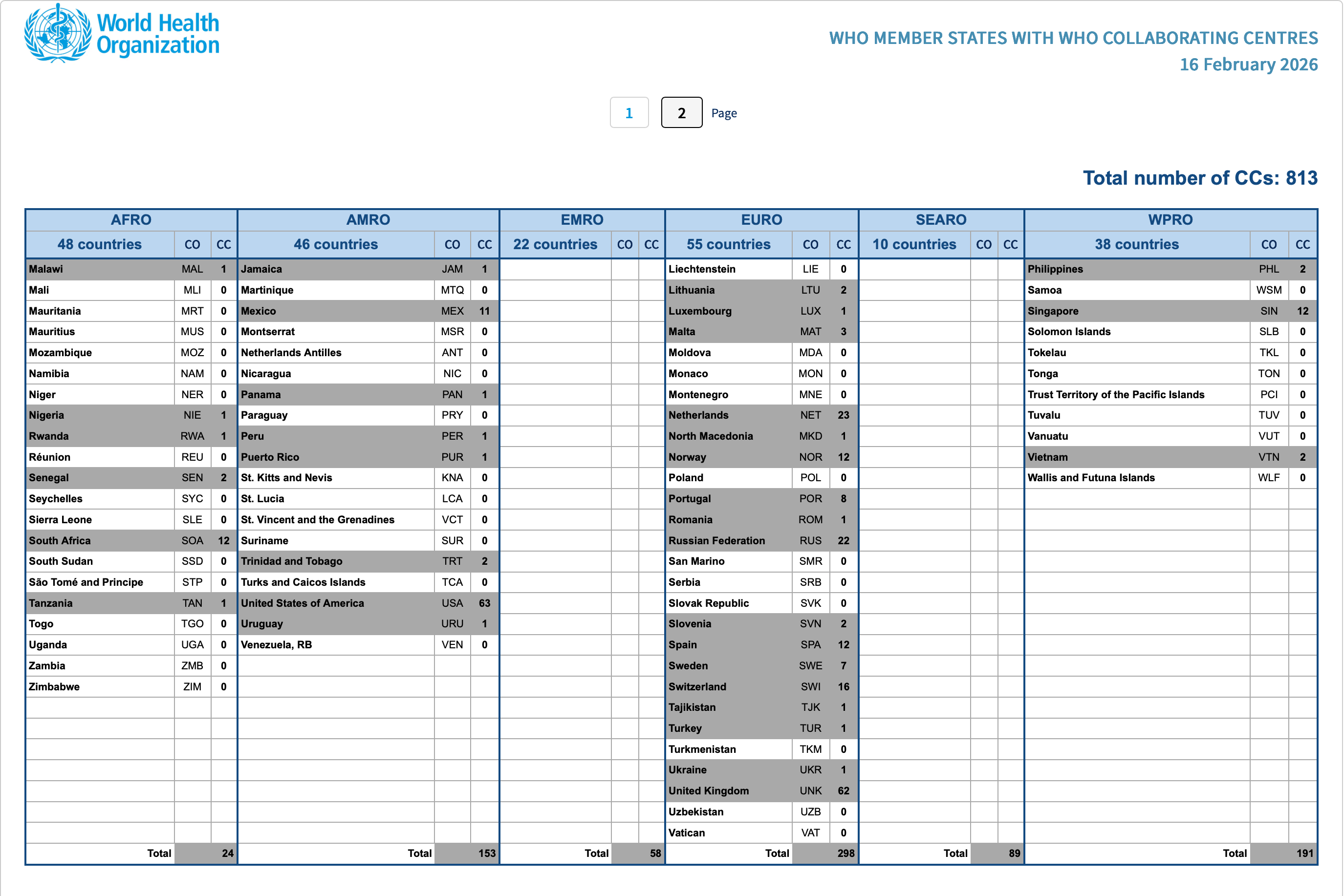
At the time of writing (16th February 2026), WHO’s database shows the US has 63 active Collaborating Centres — despite having technically exited the WHO on 22nd January. The UK has 62.
Furthermore, in terms of sheer CC numbers, the US and UK are clearly in the lead. China is a close third, followed by India, then Australia. These top five comprise 35% of the world’s 813 CCs. And it shows how massively influential the US and UK are in terms of WHO-disseminated output — which of course includes pandemic policy and products.
Therefore, the US exit from WHO is rendered seemingly meaningless — unless all of its remaining Collaborating Centre contracts are terminated. But as Section 1.13 of the US report tells us, the situation has not been made clear:
“Given that the contracts are between the WHO and the institutions designated as CCs, whether this extensive and reciprocally influential relationship will be impacted (by the US’s departure) has yet to be elucidated. Of the four CCs designated in 2025, three were designated after the US issued its notice of withdrawal.”
Expansion by stealth: how WHO’s influence is deepened and strengthened by the Collaborating Centre model
The two reports highlight some troubling features in this system of ‘partnerships’. It may be a cliché to say so, but the devil truly is in the detail.
1. The number of new WHO Collaborating Centres accelerated in the Covid and post-Covid era.
In the UK, an astonishing half of its active CCs were designated since 2021. In the US, more than a third were designated from 2020 onwards. This may well arouse suspicion as it begs the question: why the surge?
2. Contracts are dominated by ‘WHO Request’ and ‘Support WHO’.
This suggests that WHO is deploying these institutions in order to implement its required agendas. In other words, this is policy outsourcing in disguise.
It is important to note the reciprocal relationship between WHO and its Collaborating Centres. However, this is far from being an assuredly wholesome ‘partnership’ in which objective, independent expertise and best practice is shared for the good of humanity. Instead, there is a huge question mark surrounding the convoluted layers of funding, influence, and the behind-the-scenes involvement of sketchy but powerful bodies.
“These collaborations are two-way: the US/UK institutions not only work with WHO, they influence and shape WHO’s health security agenda, while the WHO’s agenda also affects US/UK policies and practices.”
—Section 1.1 (in both USA and UK reports)
3. Subject areas are heavily dominated by two macro-areas.
These are Communicable diseases/infection/pandemic and General health systems/policy.
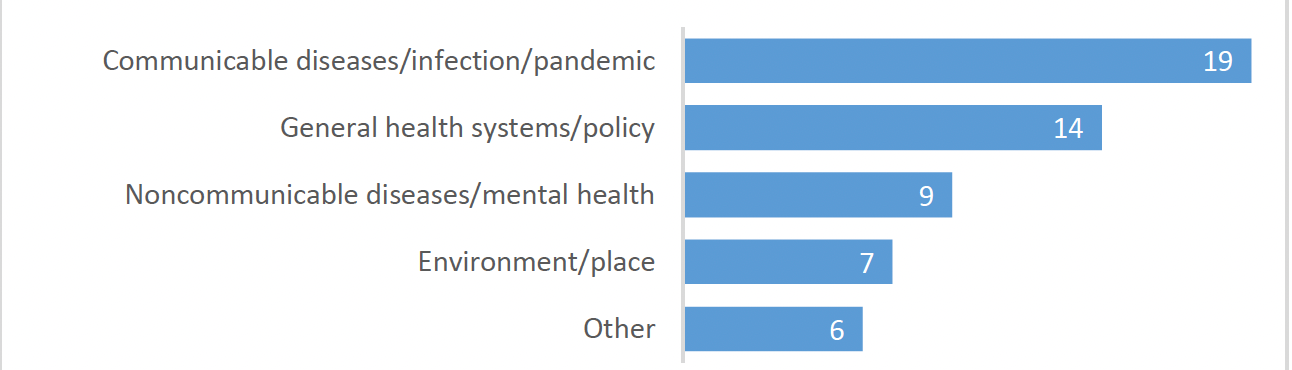
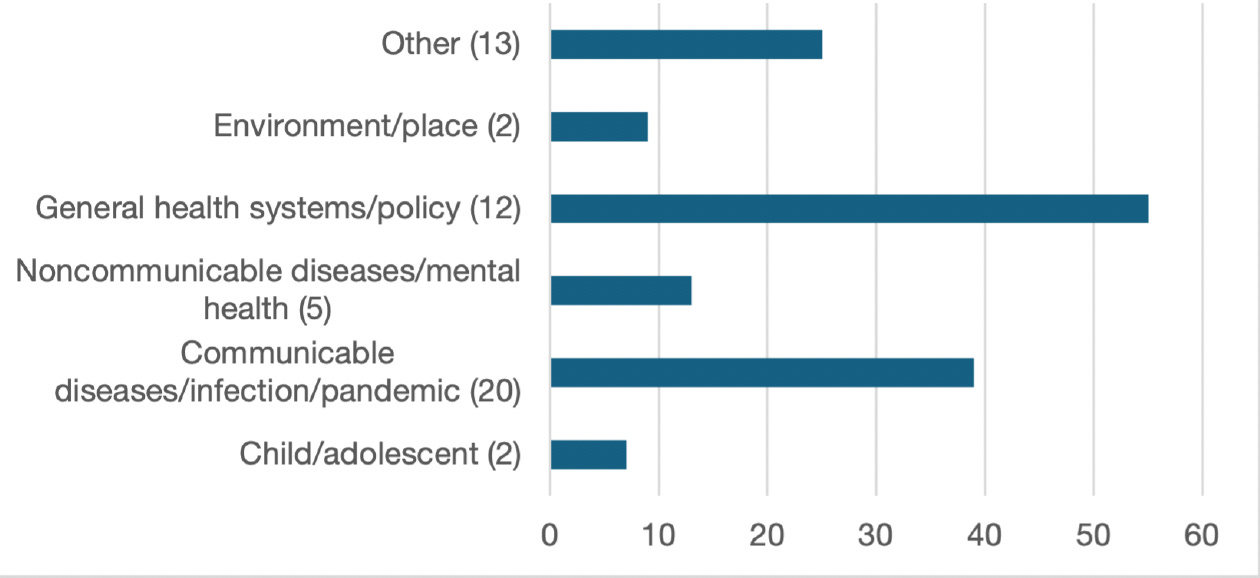
One might raise an eyebrow at the overwhelming emphasis on communicable diseases and global systems/policy. For this dual fixation maps neatly onto two of WHO’s most cherished projects: the Pandemic Agreement and the Amended International Health Regulations.
4. Certain activity types are prevalent.
Both reports note that ‘training and development’ and ‘product development’ are the predominant activity types. It is worth noting that ‘product development’ refers not only to tangible items such as biological products and equipment, but also to guidelines, diagnostics and methodologies.
Why does this matter? Because these activities shape professional and regulatory norms. Coupled with the heavy emphasis on global systems and policy as outlined above, this becomes a subtle means of generating widespread policy alignment.
5. The system is convoluted, and transparency is missing.
Contracts are between WHO and the ‘partner’ institutions. Hence they can fly under the radar for years, bypassing any kind of public scrutiny or accountability.
It is interesting when institutions do not explicitly acknowledge their WHO Collaborating Centre status on their websites. One example is the US’s National Institute for Occupational Safety and Health (NIOSH) — as noted in Section 5.6 of the US report. After considerable searching on the NIOSH website, it seems the only mention of its Collaborating Centre status is tucked away on a remote page referring to a 2016 publication. Yet it remains an active CC. Why would NIOSH —along with other institutions— sooner downplay its connection with WHO, rather than emblazon it proudly?
To complicate matters further, as well as ‘straightforward’ CC status, there are additional organisational strata baked into the WHO model. In the Americas, the Pan American Health Organisation (PAHO) adds an extra regional layer — i.e. it serves as another channel by which WHO can operate. And let’s not forget GOARN (WHO’s Global Outbreak Alert and Response Network). Several key WHO Collaborating Centres are also GOARN partners: this includes the CDC, John Hopkins University and the University of Texas Medical Branch.
And those that were discontinued…?
The ~800 active WHO Collaborating Centres are just one part of the story. There are many others which are no longer active. It is important not to overlook these, as their scope, subjects and types of activity can cast considerable light on WHO’s evolving operations and priorities.
One to note is SWI-61, the WHO Collaborating Centre for e-Health, based at Hôpitaux universitaires de Genève in Switzerland. This CC was designated for fifteen years, finally terminating on 5th January 2025. Included in its General Scope is: “Support WHO activities for the implementation of the global strategy on digital health.” The available evidence indicates that SWI-61 was an original and leading CC on digital health worldwide.
The tentacles of ‘public health’ — and questions to keep asking
There are many reasons to be concerned about WHO overreach and the Covid-style public health tyranny which, by now, we are all too familiar with. The two reports substantiate such concerns.
For example, this is from Section 1.7 of the UK report:
“The UK Health and Security Agency (UKHSA) has contracts for 9 (15%) of the CCs. Other UK government institutions are involved in another 9 contracts (15%), including Public Health Scotland and Public Health Wales (2 contracts each).”
And from Section 1.7 of the US report:
“The oldest of the CCs still operating, the WHO CC for Surveillance, Epidemiology and Control of Influenza … began in 1956. The responsible institution is the Influenza Division of the Centres for Disease Control and Prevention (CDC). This WHO CC played a significant role in COVID-19 surveillance, tests and vaccines.” (Emphasis mine.)
If we are to counter the encroaching overreach, we need to keep investigating and shining a light where there is shadiness and obfuscation. Here are some questions to keep in mind:
How are these WHO Collaborating Centre ‘partnerships’ authorised and regulated — and by whom?
How are they funded?
What exactly are the deliverables which are created ‘at WHO request’?
How do these deliverables feed into wider policy, systems or training?
Is the public-facing database transparent and trustworthy?
To access the WHO Collaborating Centres Database, go to https://who.my.site.com/ecc/s/
World Council for Health will continue shining a light and searching for answers, and stands for a Better Way.
To read our introduction to WHO Collaborating Centres:

Acknowledgements:
The World Council for Health reports cited in this article were prepared by volunteers David Abbott and Fiona Wood CA, based on extensive groundwork by Lucinda van Buuren (WCH Nursing and Midwifery Coordinator), with input from Dr Tess Lawrie (Director, EbMC2 CIC).
Please watch this important video message from Dr Tess Lawrie:

Disclaimer:
This article is not intended to be used in place of individual medical advice. It cannot be used to diagnose illness or access treatment. Individuals may use the materials provided by World Council for Health to complement the care provided by their qualified, trusted health professionals. All information provided by World Council for Health or in connection with its website is offered to promote consideration by individuals and their trained healthcare providers of various evidence-based prevention and treatment options. The information on this website is for general informational purposes and is not a substitute for medical advice. Errors and omissions may occur.