


Evidence Accumulates Connecting Covid-19 Vaccines and Cancer
It's time to stop the mRNA vaccinations because there are already too many safety signals!

On Monday 6 May 2024, World Council for Health (WCH) Steering Committee member Christof Plothe, DO had an in-depth interview with Dutch molecular biologist Dr Maarten Fornerod about current investigations into the carcinogenic potential of the SARS-CoV-2 spike protein, whether the source is infection or injection. Dr Fornerod has worked at the European Molecular Biology Laboratory and the Netherlands Cancer Institute and is a scientific advisor and board member of the Netherlands Doctors' Collective.
Increased cancer mortality after the Covid-19 booster in Japan
The first part of the interview focused on a peer-reviewed study from Japan, published in the journal Cureus on 8 April 2024. Japan is one of the most vaccinated countries in the world, having recently finished their seventh population-wide round of mRNA injections. This large retrospective Japanese study investigated age-adjusted cancer mortality.
After the third mRNA lipid nanoparticle vaccine dose, mortality figures revealed an increase in cancer-related deaths in 2021 and 2022, but not in 2020.
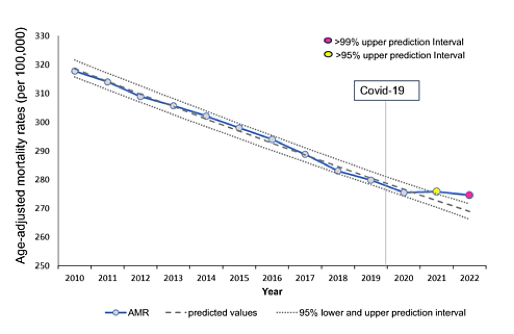
In Japan, between 2010 and 2020 (when the Covid-19 event happened) there was a slow decline in age-adjusted mortality rates (AMRs) from cancer. But in 2021 and 2022 there was a significant deviation from this downward trend. The significance level in 2022 (>99%) was greater than in 2021 (>95%).
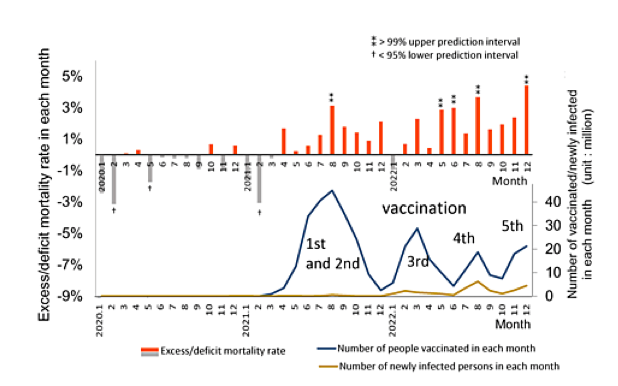
This graph represents excess monthly mortality rates from all cancers in Japan between January 2020 and December 2022. Not only was there hardly any excess mortality in 2020, but mortality actually declined (grey bars). After 2021 excess mortality (red bars) increased, rising to a maximum of about 5% by the end of 2022.
Mortality was plotted together with the first five rounds of vaccination in Japan. In the diagram, the double asterisks mean that there is a statistically significant correlation in time between vaccination and mortality.
Increase in certain types of cancers
The researchers also looked at which types of cancer increased during the period 2020-2022.
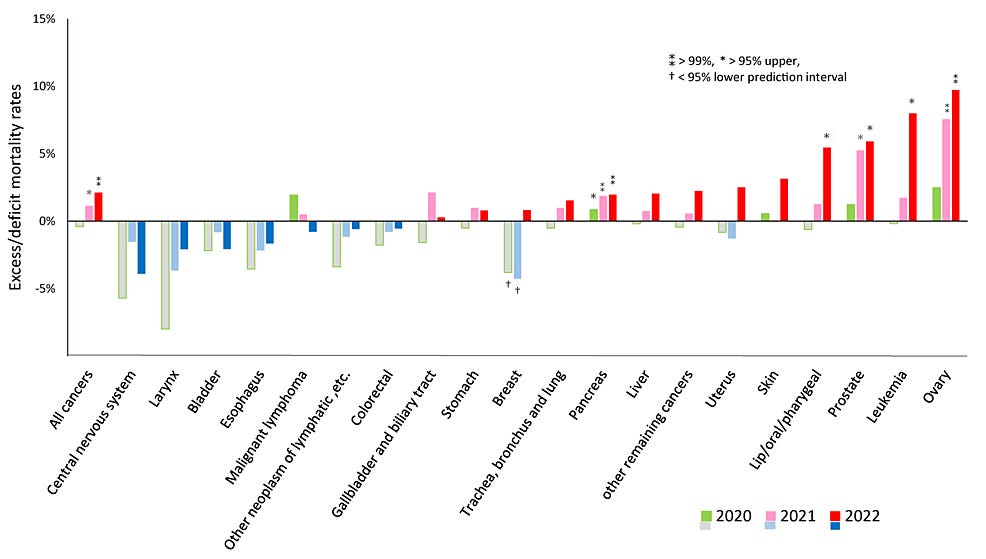
The Y-axis of this graph represents the excess or deficit in mortality from all types of cancer. It is important to note that not all types of cancer increased in frequency, and some in fact declined. Where the symbol (**) indicates statistical significance, there is a greater likelihood that the excess or deficit mortality is real.
Of the 20 types of cancers monitored, five showed significant excess mortality, namely leukaemia, ovarian, prostate, lip/oral/pharyngeal, and pancreatic cancers. There was a significant deficit in breast cancer mortality in 2020 and 2021, which then shifted to excess mortality, although this was not statistically significant. Note that very few types of cancer increased in 2020.

Interpreting the Japan study
One possible explanation for increases in cancer is that the Covid crisis may have caused this due to delayed care, stress, or unhealthy behaviours, such as people being confined to their rooms, eating unhealthy food, and watching too much television.
More worryingly, though, is the possibility that the mRNA ‘vaccines’ may have increased cancer deaths, as suggested by the timing of the first booster (third injection) coinciding with the increase in specific types of cancers.
There is evidence – some of it strong and some less so – that the Covid-19 mRNA ‘vaccines’ have carcinogenic side effects.
What evidence is there that the Covid-19 mRNA ‘vaccines’ may be carcinogenic?
Some of the strongest indicators that these ‘vaccines’ may be carcinogenic include:
Clinicians have observed an increase in cancer after mRNA vaccinations or boosters. Some case reports have been anecdotal, but those from clinicians should be taken seriously due to their experience.
There is evidence that the mRNA vaccines are immunosuppressant. Increases in IgG4 levels and suppression of the immune system repress the body’s defence against cancer.
The spike protein is known to activate the oestrogen receptor pathway (see below).
DNA contamination of the mRNA vaccines is a genotoxic risk, which in turn is a carcinogenic risk.
According to the above, there is no doubt that these mRNA ‘vaccines’ pose a carcinogenic risk. The question is, how great is that risk? And as they clearly pose a safety signal, why is the vaccination campaign continuing?
Spike protein activates the oestrogen receptor pathway
In 2022, a paper in Science Advances demonstrated that spike protein binds strongly to human oestrogen receptor alpha (ERα), causing ERα-dependent cell proliferation. Depending on the context, the purified spike could either activate or inhibit the oestrogen response. Spike protein increased cell proliferation in the oestrogen-responsive MCF-7 breast cancer cell line, but not in a cell line that was non-responsive to oestrogen. The researchers also showed that raloxifene, an oestrogen receptor antagonist, blocked this effect.
Because a specific part of the spike protein combines with the oestrogen receptor, the cancer risk could theoretically be reduced by modifying that part of the spike. This was, in fact, suggested in the Discussion section of a preprint of this article posted in May 2022. However, when the paper was published in November 2022, this sentence had been removed. Was this article censored due to possible concerns that it might contribute to vaccine hesitancy? It is highly unusual for an editor to request removal of a comment from the Discussion, as these are simply the author’s thoughts and opinions, with which the reader is free to agree or not.

Weaker arguments regarding carcinogenicity
Dr Fornerod identified two more possible mechanisms whereby spike protein could promote the development of cancer; however, the data in these cases is not as convincing:
Interaction of spike protein with BRCA and p53, and the possible effect on MDM2
‘Stimulation’ of cancer growth by N1-methyl-pseudouridine (m1Ѱ)
In the first case, the paper has not yet been peer reviewed but can be found on the Preprint Server for Biology, bioRχiv: SARS-CoV-2 spike subunit inhibits p53 activation Receptor DR5 and MDM2 proteins in cancer cells. In the experiment the authors conducted, the p53 molecule was not found to interact with the spike protein. Furthermore, there was no significant decrease in p53 or MDM2 in the presence of spike.
The second paper, Review: N1-methyl-pseudouridine (m1Ѱ): Friend or foe of cancer, reviews unpublished data claiming that the presence of m1Ѱ (the artificial base in the mRNA for spike protein) stimulates cancer growth. In this study, despite the conclusion stating that it showed that m1Ѱ promoted tumour growth there was actually no visible difference between tumour development in the lungs of mice that had received mRNA containing m1Ѱ and the controls that had not. Dr Fornerod warned that it is important to look directly at the data and not just the conclusions of these papers.
Despite these two examples of weaker evidence, Dr Fornerod concluded: It is time to stop the mRNA vaccinations because there are already too many safety signals.
We need a Better Way!
As Christof Plothe observed, testing for carcinogenicity is required before any medication is released, but this was never done in the case of the mRNA shots. There were no long-term safety data, no genotoxic studies, and no carcinogenic studies, not even in mice. This was clearly irresponsible. It was also of concern that early treatments for Covid were denied for almost a year, and instead people had to wait for a vaccine to be produced.
The Covid event drew attention to the fact that there is something seriously wrong with the fields of science and medicine, with rampant corruption, censorship, and misinformation. Having recognised the extent to which these systems are impaired, it is high time for the Better Way!
If you find value in this Substack and have the means, please consider making a contribution to support the World Council for Health. Thank you.
